
Over the last fifteen years there has been a shift away from image intensifiers (IIs) towards flat panel detectors (FPDs) in the surgical C-arm market. Charge-coupled device (CCD) sensors have been a key component of camera lens assemblies that, together with an image intensifier tube (II), form the Radiology Imaging Unit (RIU) used for X-ray imaging in C-arms for decades.

Image CMOSline C-arm courtesy of Ziehm Imaging https://www.ziehm.com/en/products/c-arms-with-flat-panel-detector/ziehm-vision-fd.html
The closure of factories producing image intensifier tubes1 and increasing demand for high-end features, such as 3D imaging, have led to a move away from using II-CCD RIUs in the dynamic imaging X-ray market and the adoption of FPDs. This trend means that systems manufacturers have started to explore alternative technologies and three main flat panel detector technologies have emerged. These are amorphous silicon (a-Si), indium gallium zinc oxide (IGZO) and complementary metal-oxide semiconductor (CMOS).
What are the advantages and weaknesses of a-Si, IGZO and CMOS in the surgical C-arm market and which technology will lead the way?
a-Si
a-Si is the amorphous, non-crystalline form of silicon used for solar cells and thin-film transistors (TFTs) in flat panel liquid-crystal displays (LCD) and televisions. Over the last twenty years a-Si FPDs have become dominant in medical and industrial X-ray imaging. A-Si FPDs are used for both static and dynamic applications, but their largest application is static general radiography, e.g. for diagnostic orthopaedic imaging and chest X-ray.
Advantages of a-Si:
A-Si is a key technology used in displays, which are produced in high volumes in large factories known as ‘fabs’. The latest Gen 10.5 a-Si display fabs use enormous 2940 x 3370 mm glass substrates, whereas most CMOS fabs produce 200 mm or 300 mm diameter silicon wafers. A-Si FPDs benefit from the economies of scale of the display industry and the image sensors used in a-Si FPDs are mainly fabricated in large display fabs in Asia, sometimes using older display fabs that are no longer competitive for the production of high-end displays. This makes a-Si a cost-effective option, especially in the larger formats such as 430 X 430 mm detectors used for chest X-ray. They are also better suited to high dose exposures than IIs, because of their high saturation dose.
Disadvantages of a-Si:
a-Si does not perform well with low dose exposures because of its relatively high read noise and has a slower pixel readout than II or CMOS. Because of its slower readout, a-Si cannot support smaller pixels, e.g. 100 μm in high frame rate dynamic imaging. This limits its ability to achieve both fast readout for dynamic imaging at the same time as high resolution needed for certain fluoroscopy applications such as Cochlear implants. For the dynamic applications that C-arms are mainly used for, these limiting factors mean that the optimal speed and resolution cannot be achieved.
Even with larger pixel sizes the performance of the current generation of a-Si FPDs is limited by the a-Si thin film transistors (TFTs). Due to the low electron mobility of a-Si, it is necessary to use large TFTs (with large parasitic dataline capacitance) and this leads to an increase in electronic noise. The electronic noise of a-Si FPDs is high enough to have a significant impact on image quality in low dose fluoroscopy2.
The biggest problem with a-Si is the relatively high electronic noise, which cannot match the low noise of IIs and CMOS X-ray detectors, leading to increased radiation dose for both clinicians and patients in low dose fluoroscopy.
The radiation exposure of clinicians working with surgical C-arms is a serious issue. A study in the American Journal of Roentgenology notes, “We observed elevated risks of brain cancer, breast cancer and melanoma among technologists who performed fluoroscopically guided interventional procedures”3. Reducing the radiation exposure of clinicians and patients is an important goal of C-arm manufacturers.
A-Si also has significant image lag, which is undesirable in fluoroscopy and 3D CT imaging. This issue can be mitigated by real-time image correction algorithms.
IGZO
Indium gallium zinc oxide (IGZO) flat panel detectors are another potential option for surgical C-arms. IGZO thin-film transistors (TFTs) were developed in the display industry about fifteen years ago to enable higher frequency displays.
Advantages of IGZO:
IGZO TFTs have an electron mobility that is <10x higher than a-Si2, which facilitates a reduction in the size of the TFT while also reducing the pixel discharge time. This results in an increase in the detector readout speed. Improving the readout speed is particularly important in achieving adequate frame rates in dynamic detectors with a pixel pitch of around 100 μm.
As IGZO TFTs can be made smaller than a-Si TFTs they offer significantly improved switching performance. As a consequence, pixels become more sensitive, can provide faster readout and detector resolution can be increased. Like a-Si, IGZO panels are available from large display fabs and are cost effective with sizes ranging from 150 mm2 to 430 mm2 for medical applications. IGZO detectors fall somewhere between high dose a-Si, on the one hand, and low dose CMOS detectors and IIs on the other hand when used in low dose fluoroscopy. They can acquire a usable image at equal or lower X-ray dose compared to a-Si. They can operate at higher frame rates and with higher resolution than a-Si detectors but slower than CMOS detectors.
Disadvantages of IGZO
In terms of performance IGZO detectors are not as good as CMOS detectors, but manufacturers are promising a lower price point. This makes them a good alternative to IIs and a-Si detectors. However, FPDs based on IGZO technology are very much in their infancy and this new kid on the block needs to prove that it can achieve the claims being made and be reliable in time and with X-ray dose. IGZO is less tolerant of X-ray radiation than a-Si and, as a result, is not suitable for industrial radiography. It is not known what the lifetime of IGZO products will be in surgical C-arm applications, but this is a concern.
In a 2019 research report by Yole Development they state that “IGZO have long been seen as a … ‘high performance/low-cost’ TFT technology … but a key issue is the lack of supply chain readiness”. Although, multiple display manufacturers have begun to launch IGZO panels for X-ray detection, IGZO does not share the production maturity and proven reliability of a-Si and CMOS for X-ray imaging.
IGZO typically has some image lag in the sensor but less than a-Si. Image lag is undesirable in fluoroscopy and 3D CT imaging.
CMOS

CMOS (complementary metal-oxide semiconductor) is the semiconductor technology used in most of today's computer microchips and image sensors. CMOS image sensors (CIS) are used in mobile phone cameras, compact cameras, video cameras and numerous machine vision applications. CMOS flat panel detectors for surgical C-arms were first launched in 2009 by the UK company Dexela (subsequently acquired by the US company PerkinElmer Inc) and introduced in mini C-arms the following year. CMOS was first used in full sized C-arms in 2017 with the launch of CMOS products by Ziehm Imaging and GE Healthcare. The technology has seen a strong level of growth in the dynamic X-ray imaging market, taking close to 100% of the mini C-arm market and most of the full sized C-arm market in developed economies. IIs still play an important role in the surgical C-arm market, especially in developing economies.
Advantages of CMOS
CMOS FPDs have a higher readout speed and lower noise than a-Si and IGZO due to the much higher electrical charge mobility in crystalline silicon and the CMOS active pixel sensor (APS) architecture. By lowering the noise floor, the low dose Detective Quantum Efficiency (DQE) is significantly improved and X-ray detection is achieved even at very low dose levels. CMOS FPDs are able to simultaneously yield better resolution and better contrast for the highest diagnostic image quality available. This results in a reduction of radiation dose to the patient and clinicians in low dose fluoroscopy in comparison with a-Si detectors.
CMOS image sensor technology also allows multiple gain modes to be implemented at the pixel level allowing different modes of operation for high dose and low dose applications, such as 3D CT imaging (high dose) and low dose fluoroscopy.
CMOS image sensors have virtually no image lag in the sensor itself, although the scintillator layer that converts X-ray photons into visible light does have some afterglow.
Disadvantages of CMOS
While CMOS detectors have the best performance characteristics (including resolution, speed and low dose image quality), the cost of the CMOS sensors results in a high cost for larger panels, e.g. 310 mm2. This is due to the relatively high cost of CMOS wafers compared to a-Si or IGZO image sensors.
Although CMOS image sensors are vulnerable to radiation damage by X-rays, CMOS X-ray detectors used in surgical C-arms are protected by a fibre optic plate (FOP), which adds additional cost but improves image quality and product lifetime.
Conclusion
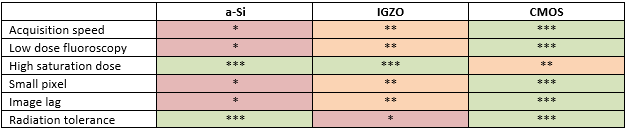
As we can see in the table below CMOS has significant advantages in the race to replace IIs in the C-arm market and is the clear winner for high performance systems whereas IGZO and a-Si have a cost advantage for value systems. (***=best in class)
1. In the last 6 years we have witnessed ON Semiconductor, formerly Kodak closing one of its CCD factories, prior to that Sony’s CCD operations were also shut down. Argus Imaging and Thales have also stopped manufacturing image intensifiers.
2. ‘Analysis of a new indium gallium zinc oxide (IGZO) detector’, Steven Freestone, Richard Weisfield, Carlo Tognina, Isaias Job, Richard E. Colbeth.
3. Rajaraman, P. et al. (2016) ‘Cancer Risks in U.S. Radiologic Technologists Working With Fluoroscopically Guided Interventional Procedures, 1994-2008’, AJR. American journal of roentgenology, 206(5), pp. 1101–1108; quiz 1109. doi:10.2214/AJR.15.15265.
4. ‘Mobile C-Arm with a CMOS Detector: Technical Assessment of Fluoroscopy and Cone-Beam CT Imaging Performance’, Niral M. Sheth, Wojciech Zbijewski, Matthew W. Jacobson, Godwin Abiola, Gerhard Kleinszig, Sebastian Vogt, Stefan Soellradl, Jens Bialkowski, William S. Anderson, Clifford R. Weiss, Greg M. Osgood, and Jeffrey H. Siewerdsen.


